科技工作者之家
科界APP是专注科技人才,知识分享与人才交流的服务平台。
科技工作者之家 2020-03-17
来源:BioArt
Cancer Cell :陈翔/刘洪合作揭示腺苷调控肿瘤PD-L1新机制——为黑素瘤患者PD-1单抗治疗提供新诊疗策略
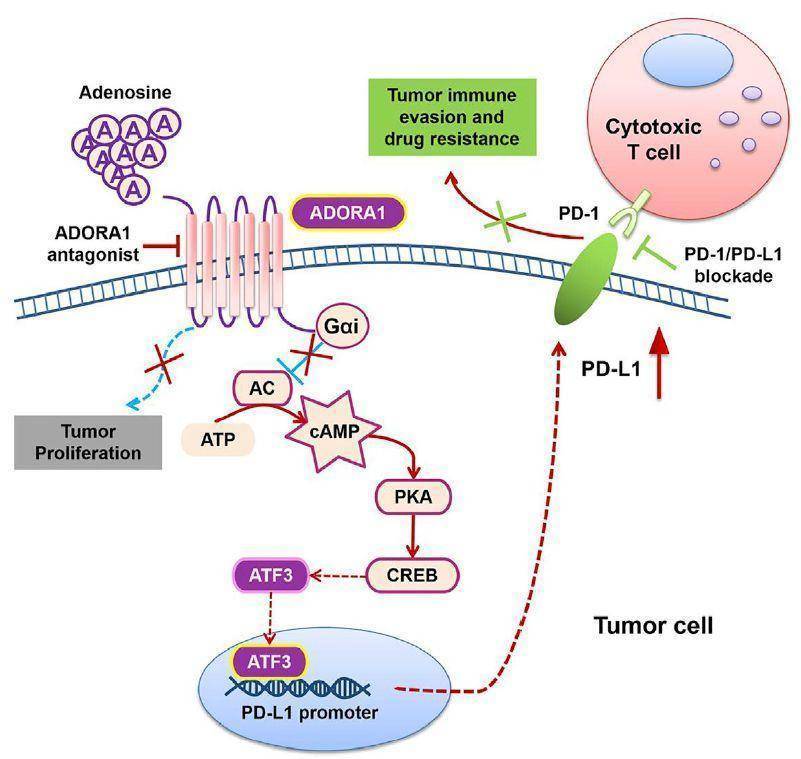
腺苷是构成机体能量来源ATP的核心代谢物。作为一种重要的内源性信号分子,腺苷的水平受到胞外核苷酸酶(CD73)、腺苷脱氢酶(ADA)、腺苷转运通道(ENT)、以及调控上述分子的关键转录因子如缺氧诱导因子(Hif1a)等多种因素影响。腺苷可作为配体,通过结合4种G蛋白偶联受体 (ADORA1, ADORA2A,ADORA2B,ADORA3) 参与调控细胞凋亡、细胞增殖、血管舒张、心脏节律、炎症等多种生理和病理过程,是当今研究的热点【1,2】。
皮肤黑素瘤是由黑色素细胞异常增殖所导致的恶性肿瘤,居皮肤肿瘤致死原因的首位【3,4】,其可独立发生与皮肤、黏膜及葡萄膜,具有侵袭力强、易转移、易复发等特点。在我国,最多见的皮肤黑素瘤临床类型为肢端型及黏膜型【5,6】,且以每年3-5%的发病速率快速增长,晚期皮肤黑素瘤2年生存率为15%,5年为5%,恶性程度极高【7】。除了采用传统手术、辅助性干扰素,常规化疗和靶向治疗等治疗手段之外【8-14】,近年来,以抗程序性细胞死亡蛋白1 (PD-1) 及其配体程序性死亡配体1 (PD-L1)相互作用为主的免疫检查点阻断疗法在黑素瘤治疗方面有了革命性进展【15-17】。2018年诺贝尔生理学或医学奖授予了肿瘤免疫检查点抑制剂,且免疫治疗正迅速广泛应用于皮肤肿瘤、肺癌、结直肠癌、乳腺癌等多种实体瘤的临床治疗。但随着研究的深入,结果显示该免疫疗法总体响应率仅不40%【18,19】,且有效筛选黑素瘤患者进行免疫治疗的评估策略缺失是临床上非常棘手的问题。因此,探究导致PD-1单抗治疗无应答的免疫逃逸分子机制、开发筛选免疫治疗有效患者的高效策略、研发提高患者应答率的新治疗方法迫在眉睫。
2020年3月16日,中南大学湘雅医院皮肤科、中南大学湘雅个体化肿瘤免疫治疗临床研究中心的陈翔教授团队与刘洪教授团队合作在Cancer Cell杂志上发表题为ADORA1 inhibition promotes tumor immune evasion by regulating the ATF3-PD-L1 axis的研究论文,该研究首次揭示了腺苷信号通路ADORA1-ATF3轴调控肿瘤PD-L1的分子机制;提出了ADORA1靶向拮抗剂联合PD-1阻断剂有效治疗黑色素瘤的新策略;并鉴定出了预测PD-1阻断剂治疗效果的可靠筛选方法。
在本项研究中,团队通过采用基因编辑、靶向小分子化合物干预、高通量测序结合生物信息分析的方法,率先揭示了抑制腺苷ADORA1-cAMP信号轴,可调控黑素瘤细胞中关键转录因子ATF3表达水平、上调黑素瘤细胞PD-L1的表达,促进杀伤性CD8+T细胞的耗竭,进而促进肿瘤免疫逃逸。在功能上,通过临床前研究证明了ADORA1靶向拮抗剂可以增强PD-1单抗治疗黑色素瘤等免疫健全小鼠模型的疗效。通过回顾性分析接受抗PD-1单抗治疗患者的治疗前的肿瘤组织样本,发现了肿瘤组织中ADORA1低,ATF3高或PD-L1高的患者应答率更高,预后更好。这一系列原创性研究成果为皮肤黑素瘤等肿瘤患者的PD-1单抗治疗提供了新的诊疗策略。
据悉,这项研究的第一作者和通讯作者单位均为湘雅医院皮肤科。刘洪教授和匡欣薇博士后为共同第一作者;陈翔教授和刘洪教授为共同通讯作者。这一由湘雅医院皮肤科团队主导的原创性研究成果对于黑素瘤等肿瘤患者的诊疗具有深远的指导意义。
原文链接:
https://doi.org/10.1016/j.ccell.2020.02.006
参考文献
来源:BioGossip BioArt
原文链接:http://mp.weixin.qq.com/s?__biz=MzA3MzQyNjY1MQ==&mid=2652482289&idx=4&sn=f40d3d308a1d11e8dc00e7d602dde60d&chksm=84e23945b395b053ffec921926a9761f453d44f90ee3b802e2354597e390982bc385007b89ea&scene=27#wechat_redirect
版权声明:除非特别注明,本站所载内容来源于互联网、微信公众号等公开渠道,不代表本站观点,仅供参考、交流、公益传播之目的。转载的稿件版权归原作者或机构所有,如有侵权,请联系删除。
电话:(010)86409582
邮箱:kejie@scimall.org.cn

肿瘤治疗新技术: 不同免疫细胞“组团”,识别多种抗原
Nature Medicine:肿瘤细胞利用MAPK通路抵抗TRK抑制剂治疗
失去细胞核的细胞在3D环境中举步维艰
每日会讯丨黑素瘤免疫治疗的研究进展及临床设计
用皮肤细胞恢复视力



以浆细胞样树突状细胞为治疗标靶可减轻皮肤型狼疮症状

从健康细胞到癌细胞,或许只需要几个突变
一个小小的细胞就有多达4200万个蛋白质分子
黑素瘤是有隐形翅膀的恶性肿瘤

肿瘤免疫治疗丨调节性T细胞及其应用


科界APP是专注科技人才,知识分享与人才交流的服务平台。
 微信
微信
 京公网安备11010202008424号
京公网安备11010202008424号